Phone: 085912 91896 Email: info@spinespecialist.co.in
Endoscopic Spine Surgery in Mumbai
When is endoscopic spine surgery usually considered?
Patients usually consider endoscopic spine surgery when persistent sciatica, slipped disc symptoms, or nerve-related leg pain continue despite medicines, physiotherapy, or spinal injections. It is a minimally invasive spine procedure performed through a small incision using a camera-guided endoscope, allowing targeted treatment of the affected spinal level with minimal disturbance to surrounding tissues. In selected cases, this approach helps relieve nerve compression while reducing post-operative discomfort and allowing earlier movement compared with conventional open spine surgery.
What is endoscopic spine surgery?
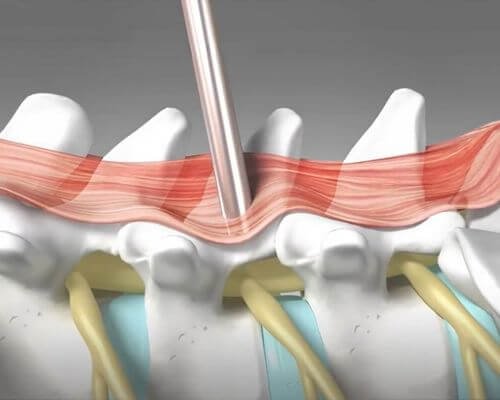
Endoscopic spine surgery is a keyhole spine procedure performed through a small incision, usually around 8–10 mm, using a thin endoscope fitted with a camera and light source.
The camera projects magnified images of the surgical field onto a monitor, allowing precise removal of the disc fragment, ligament, or bone pressing on the nerve.
Because the surgical access is narrow and focused, muscle injury is limited and surrounding structures are preserved as much as possible.
When is endoscopic spine surgery usually considered?
Endoscopic surgery is usually considered when symptoms remain persistent after conservative treatment and imaging shows a structural cause that clearly matches the patient’s complaints.
It may be advised when there is:
- leg pain caused by slipped disc
- sciatica affecting walking or sitting
- numbness or tingling radiating into the foot
- weakness related to nerve compression
- persistent lumbar pain with disc prolapse
- recurrent symptoms despite physiotherapy or medication
For many patients, surgery is discussed only after simpler treatment has failed to provide stable relief.
Which spine conditions can be treated through an endoscopic approach?
Endoscopic techniques are most commonly used for selected lumbar spine conditions where the target area can be reached safely through a small working channel.
These include:
Slipped disc
(herniated disc)
sciatica caused by nerve
root compression
lumbar canal stenosis
in selected cases
Foraminal
stenosis
Recurrent disc
prolapse
degenerative disc-related
nerve compression
Some cervical spine conditions may also be treated through endoscopic techniques when anatomy and surgical indication are appropriate.
Why does one patient need surgery while another does not?
An MRI finding alone does not automatically mean surgery is required.
Many patients have disc bulges on imaging without severe symptoms. Surgery is usually considered only when scan findings match pain pattern, neurological signs, and functional limitation.
A patient with severe leg pain, weakness, or progressive nerve symptoms may need intervention earlier, while another with similar imaging may improve with non-surgical treatment.
This is why specialist assessment matters more than the scan report itself.
How is suitability decided before endoscopic spine surgery?
Suitability is decided after combining clinical examination with imaging and symptom history.
Evaluation usually includes:
- exact pain distribution
- duration of symptoms
- numbness or weakness
- walking limitation
- nerve examination
- MRI of the spine
When symptoms and MRI findings do not fully match, additional assessment may be needed before deciding surgery.
The goal is to confirm that the compressed nerve seen on imaging is truly responsible for symptoms.
What are the main benefits of endoscopic spine surgery?
The main advantage of endoscopic surgery is that treatment is focused only on the affected area while preserving surrounding tissues.
For selected patients, this often means:
- small incision
- less muscle injury
- lower blood loss
- reduced post-operative pain
- shorter hospital stay
- earlier mobilisation
- quicker return to daily routine in many cases
The goal is not simply a smaller surgery, but precise nerve decompression with minimal unnecessary tissue disturbance.
Endoscopic spine surgery vs conventional open spine surgery
Endoscopic spine surgery differs from open surgery mainly in how the spine is accessed.
Open surgery usually requires a larger incision and wider muscle exposure. Endoscopic surgery uses a narrow working channel and camera-guided magnification.
This often leads to:
- smaller scar
- less tissue trauma
- faster early recovery
- lower wound-related discomfort
However, not every spinal condition is suitable for endoscopic surgery. More complex instability, deformity, or multilevel disease may still require another surgical method.
How is endoscopic spine surgery different from minimally invasive spine surgery?
Endoscopic surgery is one form of minimally invasive spine surgery, but the two are not identical.
Minimally invasive spine surgery includes several techniques performed through smaller incisions using specialised instruments or tubular systems.
Endoscopic surgery specifically uses a camera-guided endoscope through a very narrow channel, making it especially useful when treatment is limited to a focused area such as disc-related nerve compression.
What happens during the procedure?
After confirming the exact spinal level, a small incision is made over the affected area.
The endoscope is introduced through this opening, usually from the back or side depending on the location of the pathology. Using camera guidance and fluoroscopic imaging, the compressed nerve is identified and the disc fragment, thickened ligament, or bone causing pressure is removed.
The procedure usually takes one to two hours depending on complexity.
In many cases, patients are able to sit, stand, and walk within a few hours after surgery depending on overall condition.
What does recovery usually look like after endoscopic spine surgery?
Recovery is often quicker than conventional open surgery, but it still depends on the underlying condition, nerve irritation before surgery, and general health.
Many patients begin walking early after surgery.
For desk-based work, return often happens within one to two weeks. More physically demanding work usually takes longer.
Early recovery usually focuses on:
- avoiding bending and twisting
- controlled walking
- gradual increase in daily movement
- posture awareness
Pain often improves progressively rather than disappearing immediately.
Patients from Mulund, Chembur, Ghatkopar, Thane, Navi Mumbai and nearby areas often seek specialist evaluation when repeated medication or physiotherapy no longer provides durable relief.
Timeline
What is the expected recovery timeline after endoscopic spine surgery?
Recovery usually happens in phases rather than all at once, and the exact pace depends on the condition treated, nerve recovery, muscle strength, and the type of work a patient does.
First 24 hours
Many patients are able to sit, stand, and walk within a few hours after surgery depending on overall condition. Some are discharged the same day or the following day.
First 1 to 2 weeks
This period usually focuses on wound healing, controlled walking, and avoiding bending, twisting, or lifting. Desk-based work may be resumed gradually in selected patients.
2 to 6 weeks
Daily movement usually becomes easier during this phase. Leg pain often improves steadily, though numbness may take longer if nerve irritation existed for a long time before surgery.
After 6 weeks
Patients involved in physically demanding activity often return gradually after review, depending on strength, symptom recovery, and spinal stability.
Recovery is usually faster than conventional open surgery, but nerve healing still varies from person to person.

Like all spine procedures, endoscopic surgery has limitations and possible complications.
These may include:
- bleeding
- infection
- dural tear
- incomplete symptom relief
- recurrence of disc prolapse in some cases
The risk remains low when patient selection and surgical indication are appropriate.
How successful is endoscopic spine surgery?
In properly selected cases, endoscopic spine surgery usually provides significant relief from leg pain caused by nerve compression, especially when symptoms clearly match MRI findings.
Results depend on:
- severity of nerve compression
- duration of symptoms before surgery
- nerve recovery potential
- overall spinal condition
Patients with long-standing weakness may recover more slowly than those treated earlier.
When should surgery not be delayed?
Surgery should not be unnecessarily delayed when nerve compression begins affecting function.
This becomes more relevant if there is:
- progressive leg weakness
- foot drop
- difficulty walking
- severe persistent sciatica
- bowel or bladder symptoms
- worsening numbness
At that stage, delaying treatment can affect nerve recovery.
Frequently asked questions about endoscopic spine surgery
Is endoscopic spine surgery painful?
Because the incision is small, post-operative discomfort is usually less than open surgery, although temporary soreness is expected.
Can I go home the same day?
Some patients are discharged the same day or the following day depending on recovery and overall condition.
Is endoscopic spine surgery always better than open surgery?
No. It is useful in selected cases where the pathology can be treated effectively through a limited approach.
Can slipped disc return after surgery?
Recurrence is possible in some patients, although many remain symptom-free long term when recovery advice is followed properly.
Is every slipped disc suitable for endoscopic surgery?
No. Suitability depends on disc position, nerve compression, spinal stability, and symptom pattern.
Centers